Current Homelessness Policy Landscape
Updated March 16, 2022
Homelessness in Multnomah County - Background and Thoughts
Multnomah County Commissioner Sharon Meieran
Updated April 2, 2021
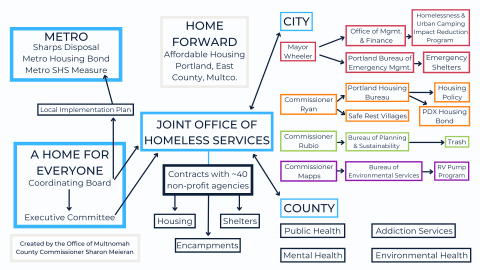
I. Landscape of orgs/entities developing homeless policy and providing services
The following agencies and services are involved in serving and developing policy for the housing/homelessness continuum (this list is not comprehensive, but describes some key players):
- A Home For Everyone (AHFE) - An initiative created in 2014 to bring community together to end homelessness in Multnomah County. AHFE comprises an executive committee (EC) made up of elected officials from Portland, Multnomah County and Gresham, along with representation from Home Forward (formerly the Portland Housing Authority), service providers, the business community, and the faith and philanthropic communities. The EC works with a diverse coordinating board (CB) and several policy-focused work groups. Together, the EC and CB were intended to set priorities and make recommendations on policies and spending for Multnomah County’s local housing and homelessness continuum of care.
- Joint Office of Homeless Services (JOHS) - Established between Multnomah County and Portland in 2016 (and funded by both, in addition to state, federal and other grant funds), JOHS administers contracts for housing and homeless services, conducts one-night homeless street and shelter counts, manages systems of care, and oversees systems reporting and evaluation. JOHS operationalizes many of the priorities established by AHFE.
- Multnomah County Health Department, including Behavioral Health Division and Public Health Division - provides support and services related to mental health, substance use disorder, street behavioral health outreach and crisis response, broader community health, harm reduction (needle exchange, Narcan), public health crisis response, infection control, vector control (i.e., rats), and more.
- Portland Housing Bureau - develops citywide housing policy to increase the supply of affordable housing and promote housing stability, and administers a broad range of federal and local resources. PHB monitors the implementation of the 2016 Portland Housing Bond. Currently, Commissioner Dan Ryan heads this bureau.
- Home Forward - Formerly the “Portland Housing Authority,” Home Forward “promotes, operates and develops affordable housing that engenders stability, self-sufficiency, self-respect and pride in its residents and represents a long-term community asset.”
- City of Portland Homelessness and Urban Camping Impact Reduction Program (HUCIRP) - coordinates cleanup of unsanctioned campsites on land owned by Portland and the Oregon Department of Transportation, coordinates services with other agencies and jurisdictions, and “creates service navigation opportunities for individuals experiencing homelessness while also facilitating the removal of hazardous items and debris from our public spaces.” Toward these aims, HUCIRP also manages the City’s One Point of Contact campsite reporting system. Recently, the Mayor’s office announced a plan to more aggressively pursue camp cleanups.
- Metro - a regional government agency serving more than 1.5 million people in Clackamas, Multnomah and Washington counties, providing region-wide planning and coordination on growth, infrastructure and development issues that cross jurisdictional boundaries. In recent years, Metro has expanded its portfolio to include significant housing work, collaborating with local cities and counties to engage the community and ask voters to support the creation of new affordable housing and services in the region.
A $652.8 million affordable housing bond measure passed in 2018 to create permanently affordable housing across greater Portland for seniors, working families, veterans and others.
Metro Supportive Housing Services measure - A measure expected to generate revenue of around $2.5 billion over ten years in the Portland metro region. These funds will “Provide for the much-needed wraparound services to help reduce homelessness across greater Portland. The program provides services for as many as 5,000 people experiencing prolonged homelessness with complex disabilities, and as many as 10,000 households experiencing short-term homelessness or at risk of homelessness.”
- Multnomah, Clackamas and Washington counties have each developed a Local Implementation Plan (LIP), setting forth system gaps and priorities for investment under the SHS measure. The LIP for Multnomah County was drafted by the Coordinating Board of AHFE and approved by AHFE’s Executive Committee, the Multnomah County Board of Commissioners, the Metro Oversight Committee, and finally the Metro Council.
- The LIP is 32 pages long, with over 100 additional pages of addenda and documents, and includes a number of broad priorities. It prioritizes identifying and addressing racial disparities in Multnomah County’s homelessness system.
- Multnomah County’s LIP acknowledges the limitations of traditional indoor congregate shelter and describes alternative shelter as one of the “most pressing needs as identified through data and by stakeholders,” along with behavioral health services.
- The LIPs for the three regional counties will be coordinated and monitored by a Metro Oversight Committee.
II. How we define and understand homelessness
There are truly as many reasons for homelessness as there are people experiencing it. For the purpose of conceptualizing the system, however, it can be helpful to consider two broad categories of people who experience homelessness (see ECO-NW study). The two categories include:
- People experiencing “transitional” homelessness, who do not have enough income to meet their housing cost burden, and may be one medical bill/car payment/job loss away from losing their housing. These individuals often need mainly rent assistance and physical housing, but may also need support services such as childcare, utility assistance, or job skills training;
- People experiencing more “chronic” homelessness, including people experiencing serious mental illness, substance use disorder, or other serious disability, who need not only deeply affordable housing, but intensive supportive services to enable them to sustain that housing.
It is important to note that, if people who fall into the first “category” don’t have their needs met, many may be at risk of becoming chronically homeless.
III. General strategic approach to “ending homelessness”
Services in Multnomah County and the City of Portland are largely provided through a network of community-based organizations contracted through JOHS. Service priorities are shaped, in part, by guidance from AHFE with an approach that drives toward three key aims: (1) Preventing homelessness; (2) emergency shelter and safety on/off the streets; and (3) permanent housing.
In general, the best way to “solve” homelessness is by preventing it from happening in the first place. JOHS employs strategies such as emergency financial assistance to help with utility bills and other basic needs, short and long term rent assistance, and other mechanisms to prevent people from losing their homes. Shelter and emergency services are geared toward providing a safe place for people to stay while they get connected to services and, ideally, transition into permanent housing. And permanent housing includes housing that is “deeply affordable” (accessible to households making 0-30% of median family income), “affordable” (accessible to households making 30-60% of median family income), and “supportive” (deeply affordable housing with wraparound services for people with severe underlying disabilities, including mental health and substance use disorder needs). It has been shown that supportive housing is the most effective permanent housing strategy for people who are experiencing chronic homelessness.
Allocation among these strategies is where tough budget choices must be made, because any resources expended on one of these strategies is unavailable to allocate to another strategy. For example, resources allocated to shelter will not be available to prevent a family from losing their apartment when they are unable to pay their utility bill.
IV. Shelter for people who are chronically homeless/living unsheltered
Historically, approaches to people living unsheltered have focused on getting people indoors into “traditional” shelters, and this is the model primarily adopted by JOHS. Traditional shelter includes congregate and semi-private living spaces in a variety of settings (serving families, adults, women, veterans, couples, people escaping domestic violence, etc.), where the goal is to transition people into permanent housing as quickly as possible. As permanent housing opportunities have become scarcer, people have been living longer and longer in shelters that were meant to offer safety during a brief stay as people transitioned out of the shelter. In addition, a few “alternative” models of shelter have been put in place, such as tiny home villages, motel-based shelters and publicly-sanctioned encampments during the COVID-19 pandemic.
It has become apparent that traditional congregate shelter does not serve the needs of many individuals for a variety of reasons: People express safety concerns about being in the shelters; they worry their personal effects, including medications, might be stolen; they have mental health issues making it difficult to be indoors in a closed space with lots of other people; people feel infantilized and dehumanized by some of the rules imposed in shelters. Another layer of challenge was introduced by the COVID-19 pandemic, which made it necessary to reduce the number of people in congregate shelter to allow for physical distancing.
V. Expanding Alternative Shelter
A broader strategy of alternative approaches to shelter has traditionally not been considered by AHFE or JOHS. However, given the significant numbers of people living outside, I have advocated for the urgent adoption of an approach that provides for an expansion and continuum of alternative strategies as we strive toward longer term meaningful change and permanent housing solutions.
One way I frame this approach is through a public health lens of “harm reduction” (please see my op-eds published in the Oregonian on this subject: Homeless crisis needs urgent public health response focused on reducing harm and Faster action needed on homelessness crisis, starting with 5 critical steps). Tragically, our region does not have the capacity to provide housing or even indoor shelter for everyone living on our streets. Therefore, the question we must urgently address is “How can we minimize the trauma, suffering, and public health and safety risks associated with unsheltered homelessness while we are working toward longer term solutions, given that people will continue to need to live outside?” This is a different/additional framing of the issue than has traditionally been considered, but I believe that the evolving landscape in our County demands an expansion beyond traditional ways of thinking, and an urgency that to date has not manifested with regard to the local crisis of unsheltered homelessness.
In addition, there is still a siloing of many programs and services that I believe prevents a true coordination and integration of approaches that could meaningfully address unsheltered and chronic homelessness. For example, camp “cleanups” (often referred to as “sweeps”) are under the purview of the city through HUCIRP, while syringe exchange and disposal are implemented through the county via Public Health. Meanwhile, mental health and addiction services fall under a separate county Division of Behavioral Health, though a few scattered programs have been administered by the city. I believe there must be coordination and integration of these systems (and more) within AHFE if we are to meaningfully address the challenging conditions facing those experiencing chronic homelessness, along with the impacts on the broader community.
VI. Vision for a short term alternative shelter continuum while we strive to end homelessness over the long term
I believe that we are facing a humanitarian crisis right now, and that it is unconscionable that people are living outside in conditions that are unhealthy, unsafe, and simply inhumane. Ultimately, we need a continuum of housing that meets people’s needs, including the provision of wraparound services, but it will take years, if not decades, to reach this goal.
As we strive for long-term meaningful change, I believe we need a continuum of alternative places people can be if they cannot be housed and they cannot or do not wish to be in traditional shelter. Please see my proposed Six Month Framework to Reduce Harm for People Living Outside for my thoughts on how we can effect real change over a defined six month period.
One approach championed by Commissioner Dan Ryan and being pursued by the City of Portland is for six “safe rest villages.” This concept is similar to some aspects of the broader framework I proposed, and I fully support these efforts. However, I believe we need to be acting more broadly, at a greater scale, more urgently, and with more coordination and true partnership between the City and County.
VII. Rays of hope
There are a number of things happening in Multnomah County and the region that give me hope that we can get to a place of meaningful change, though this change won’t happen overnight. These include the Metro Supportive Housing Services Measure, along with a few additional individual programs and opportunities that can help fill some of the tremendous gaps in our systems of housing/homelessness and behavioral health.
- Metro Supportive Housing Services Measure
As described above, each of the Portland metro-area counties has developed its own Local Implementation Plan (LIP), setting forth its system gaps and priorities for investment under the SHS measure. Throughout the development of Multnomah County’s LIP, I have advocated for prioritizing approaches that serve people experiencing chronic homelessness, and including metrics that capture this specific priority. I will continue to advocate for: (1) addressing the significant unmet needs for intensive behavioral health services; (2) prioritizing development and implementation of a strategy to urgently reduce harm and improve health, safety, and dignity for people living unsheltered while we are working toward longer term permanent housing solutions; (3) mechanisms for meaningful data collection and accountability, along with outcome measures and metrics that specifically demonstrate progress toward the goal of ending chronic homelessness; and (4) communication of information that is transparent and easily understandable. This ideally would include building out the infrastructure needed to collect data in an effective, centralized and coordinated way (including regional coordination), and providing a forward-facing dashboard that communicates progress to the public in real time.
Multnomah County’s approved LIP is targeted throughout to address racial inequity and disparities, and prioritizes investment in culturally specific and responsive services that are participant centered, trauma-informed, low-barrier, and continuously evaluated to improve outcomes.
Additional specific priority investment areas include:
(a) supportive housing services, including rent assistance and wraparound housing retention supports;
(b) an expansion of behavioral health services delivered to people whether they are unsheltered, in shelter, or in housing; and
(c) additional and more diversified emergency shelter options
(d) note: a JOHS program is currently underway to fund both capital and operational needs of some community-led sheltering options (up to 200 new shelter beds) that prioritize the needs of Communities of Color, people with behavioral health needs, and underserved geographic areas of the County.
- Additional opportunities underway in the City, County and State:
- Behavioral Health Resource Center. This is currently being developed in Multnomah County, and will essentially serve as a “living room” and more for people with behavioral health needs living in shelters or outside. People will be able to come in and be accepted for who they are. They will have access to respite, a cup of coffee, and a place to be, and they will have access to services if they want them, including things like group meetings, art therapy and music therapy, showers, laundry machines and bathrooms. The services will be peer-driven and will be culturally responsive. Right now there is nowhere for people experiencing serious behavioral health needs to go, or to be brought by law enforcement or healthcare workers or outreach providers, other than jail or an ER. This will be an alternative that supports people and meets their needs, so they can potentially avoid falling into crisis. It will also provide shelter for people with mental health needs, along with transitional housing for people leaving institutional settings such as the Oregon State Hospital, jail, or inpatient hospital units.
- Portland Street Response. This is a City of Portland effort, spearheaded by Commissioner Hardesty. In our current system, if someone is living unsheltered and experiences a mental health crisis or other serious underlying mental health need, often the only potential response is through law enforcement. This can lead to escalation of the crisis, additional trauma, and is often not effective in addressing the needs of the person experiencing the crisis or the person who called for help. Through Portland Street Response, teams of EMTs, qualified mental health service providers and peers will respond to these situations, rather than police officers. A pilot is currently underway in the Lents neighborhood, and there is an effort to expand the program throughout Portland.
- Note that there are a number of existing outreach services provided by both the City of Portland and Multnomah County, operating under a number of different departments, agencies and divisions. A mapping of some of these services was accomplished through a “Sequential Intercept Model” project in September, 2019, and the describes a wide range of outreach and crisis services which already exist, along with some prominent gaps in service. Examples of these services include:DocumentSIM Report 2019 Multnomah County (864.84 KB)
- Cascadia Behavioral Healthcare Project Respond
- Crisis outreach services
- Shelter support team
- Cascadia Street Outreach Team
- Cascadia Behavioral Healthcare Urgent Walk-In Clinic
- Portland Street Medicine
- Portland Fire & Rescue Community Healthcare Assessment Team
- Portland Police Bureau Behavioral Health Unit
- Multnomah County Sheriff’s Office Homeless Outreach and Programs Engagement (HOPE) Teams
- Cascadia Behavioral Healthcare Project Respond
- Note that there are a number of existing outreach services provided by both the City of Portland and Multnomah County, operating under a number of different departments, agencies and divisions. A mapping of some of these services was accomplished through a “Sequential Intercept Model” project in September, 2019, and the
- There was an effort to expand Portland Street Response citywide, however this degree of expansion was not funded for FY22. As the pilot continues and the needs for decriminalizing mental health issues and homelessness, along with providing alternatives to law enforcement responding to mental health crises, continue, there is an opportunity for the City of Portland and Multnomah County to collaborate in ensuring that an efficient and effective system is in place to meet the behavioral health needs of people in crisis, particularly those who are houseless.
- Behavioral Health Emergency Collaborative Network (BHECN). Initially conceived as a facility to replace Portland’s Sobering Center, this project has evolved into a much more comprehensive and coordinated vision to address mental health and substance abuse crises. Right now people experiencing behavioral health crises can be taken to one of two places: an ER or jail. Neither is effective in addressing people’s underlying needs, and neither will help break the dehumanizing cycle of ERs, jails and homelessness. BHECN will be a facility that allows for the triage, evaluation, stabilization and appropriate referral for people experiencing behavioral health crises. The facility will operate as a “hub,” with a number of “spokes” connecting people in an effective and meaningful way with the services they need in real time. This facility will be complementary to the Behavioral Health Resource Center described above, providing a place for people to go, or be brought by family members, law enforcement, emergency medical services, or Portland Street Response, when they are experiencing a behavioral health crisis. It will also address the need for a “sobering center,” but be safer, trauma-informed and more broad-based.
- Shelter To Housing Continuum Project (S2HC). Changes to City of Portland Code that allow for increased flexibility and opportunity for a variety of shelter options. This can contribute to a broader network of safer, healthier, more stable options for people experiencing unsheltered homelessness in the near term, while we work toward longer term solutions.
- Frequent User Systems Engagement (FUSE). This model recognizes that some of the people who are most vulnerable and most difficult to house are over-represented in multiple systems, including jails, homeless shelters and ERs. Through this approach, “data is used to identify a specific target population of high-need, high-cost individuals who are shared clients of multiple systems, and whose persistent cycling indicates the failure of traditional approaches. Data is also used to develop a new shared definition of success that takes into account both human and public costs, and where the focus is on avoiding institutions altogether and enable meaningful service provision and engagement, as opposed to simply offloading clients from one system to another.” I believe implementing this approach is crucial to developing strategies to coordinate support for the most vulnerable people in all of our crisis systems, and can ultimately direct us toward providing the most effective care in the most appropriate place. This can allow us to allocate our limited resources to where they can be most effective across multiple systems.
- Safe Rest Villages. Described above, up to six safe rest villages have been proposed by City Commissioner Dan Ryan to provide safe sleep structures, hygiene and case management/behavioral health services for people currently living unsheltered. The city of Portland has gone through an evaluation process to site and design these villages, which will be funded by resources allocated by the federal government for COVID-19 recovery. This is a small part of the much bigger picture, but are an encouraging first step to actively reduce harm for people living outside in real time.
- Work Group to Decriminalize Mental Illness, chaired by Judge Patrick Wolke and State Senator Floyd Prozanski. Much of Oregon’s system of mental health care is governed by state policy, and it will require significant systems and statutory changes at the state level in order to make any headway in improving this dysfunctional system. One issue in particular that has broad implications for behavioral health treatment in general is the issue of “involuntary commitment.”
Currently, under Oregon statute and as interpreted by Oregon courts, people experiencing serious mental illness cannot receive medication or other treatment unless they affirmatively agree to that treatment, or they are at “imminent risk” of harming themselves or others. This statute has been narrowly interpreted to essentially mean that people cannot be involuntarily treated unless they have a meaningful plan to immediately harm themselves or others. Unfortunately, as I have seen firsthand as an emergency physician, and also working shifts with Portland Street Medicine and as a community member, in some situations people may simply not have the capacity to make decisions regarding their own health or safety, but can still pose serious risks, including putting their own and others' lives at risk. The Workgroup to Decriminalize Mental Illness is considering ways to potentially address these issues. It is a difficult conversation, but one we need to have openly and transparently so we can devise a continuum of approaches to get people the care and services they need, even when they do not have the capacity to make these decisions for themselves.
Ways you can be involved:
- Attend AHFE Executive Committee and/or Coordinating Board meetings - you can provide public testimony at the beginning of these meetings.
- Attend Multnomah County Board meetings - you can provide up to three minutes of public testimony at the beginning of these meetings. This can be combined with others’ testimony if you want to provide a collective presentation.
- Attend Portland City Council meetings - offers an opportunity to provide public testimony similar to County meetings.
- Write to, call or meet with individual City and County Commissioners.
- Write to, call or meet with your Oregon state legislators.
- A couple of hints:
- For the City, the key people to correspond with for housing issues include Mayor Ted Wheeler and Portland Housing Bureau Director Dan Ryan, but in general it is helpful if you reach out to all the commissioners, or at least copy them in any communications.
- For Multnomah County, it is important to correspond with Chair Deborah Kafoury and your specific district representative, but in general it helps to include all the commissioners because we all are involved in decision-making.