The Multnomah County Board of Commissioners received an informational briefing on Thursday, May 16 detailing work underway at the County’s Behavioral Health Division, which oversees programs and contractors that provide recovery-based mental health and addiction services to adults, children and families.
The Behavioral Health Division’s (BHD) nearly 360 employees work with partners across the continuum of care — including health systems, coordinated care organizations, community-based organizations, law enforcement partners and peers — to implement the Community Mental Health Program, said Health Department Director Rachel Banks.
To administer the Community Mental Health Program (CMHP), said Behavioral Health Director Heather Mirasol, the division coordinates a system of behavioral health services to Multnomah County residents, which includes the uninsured and under-insured. The CMHP also requires the Behavioral Health Division to collaboratively identify needs with its partners; to ensure that residents have access to mental health crisis services 24/7; to support the effective transition of individuals from the Oregon State Hospital into new service placements; and to coordinate mental health services with public safety system partners.
“As the people charged by the Oregon Health Authority to be the Community Mental Health Program and provide these services, the Behavioral Health Division and Health Department both deliver services across the lifespan and work with other system partners who deliver services across our community,” Banks said.
While division leaders had previously presented to the Board “to describe the system that we have,” Banks characterized the process moving forward as “an opportunity to describe the sort of system that we need — bringing a population approach to our behavioral health work, which includes more primary prevention, substance use disorder continuum of care, and includes a wide variety of partners, from the Board to coordinated care organizations.”
The behavioral health system, like so many other systems of care, is facing clients with increased needs, workforce shortages and capacity issues, Banks and her fellow speakers stressed.
“We need to be building pathways, hallways or doors… from one part of the system to the next so folks are focused on the people and that they’re getting the services they need at every part of their journey,” Banks said.
So that investments, she said, “are thoughtful, maximized and focused on solving the right problem for people, at the time that they need it.”
Roles of the Behavioral Health Division
The Behavioral Health Division approaches its work through a consumer-driven, trauma-informed, racially equitable and culturally responsive lens, said Mirasol, its newly appointed director. The effectiveness of that work hinges on these core values in addition to transparency, integrity, cultural humility and stewardship.
The Behavioral Health Division includes six units:
- Community Mental Health Program
- Direct Clinical Services
- Care Coordination Unit
- Addictions and Prevention
- Quality Management Unit
- Administrative Unit, which houses the Office of Consumer Engagement.
The Community Mental Health Program, overseen and administered by the Behavioral Health Division, provides both direct services and contracted support for an “exceptional pool of community-based organizations,” said Mirasol.
The division identifies needs and collaborates with system partners to ensure the provision of service elements through financial assistance agreements with the Oregon Health Authority — whether directly or by contract, said Mirasol.
“We hold the responsibility of ensuring that Multnomah County residents have access to mental health crisis services 24/7 and to support the effective transition of people from Oregon State Hospital to new placements and services,” she said.
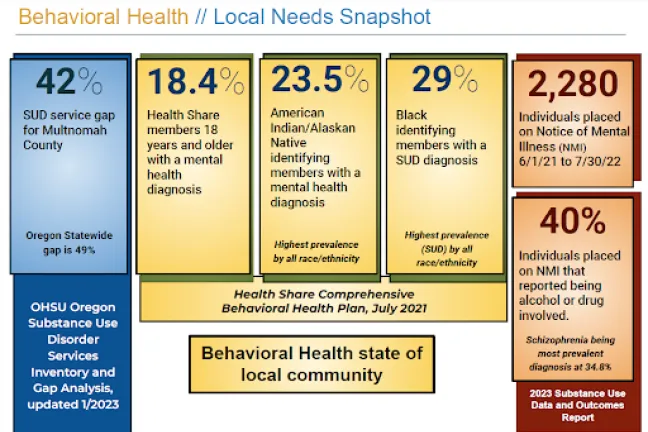
Noting that the division is “frequently asked about gaps in the capacity of substance use disorder and mental health continuums of care." Mirasol, shared a snapshot of local behavioral health needs in Multnomah County. The data was collected by Health Share of Oregon as part of a needs assessment they have been charged with maintaining since the Medicaid benefit oversight role shifted from the County to coordinated care organizations.
The Behavioral Health Division has extensive data about who it is serving — 56,000 individuals last year, Mirasol said.
She acknowledged, however, that there are challenges with identifying those who are not being served. But more resources are being dedicated to accessing this information, such as Oregon Health & Science University’s recent study with the Oregon Health Authority and the Oregon Alcohol and Drug Policy Commission on the substance use disorder continuum.
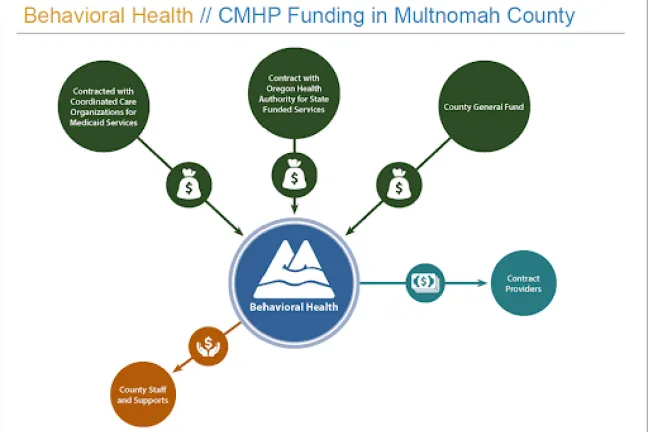
The Behavioral Health Division operates with funding from across system partners, including coordinated care organizations, the Oregon Health Authority and the County General Fund. Sixty percent of its employees are direct care providers.
The division's Direct Clinical Services includes Early Childhood, Preschool for All Mental Health, School-based mental health, K-12 Case Management and Early Assessment programs. It also includes the Gun Violence Impacted Families Behavioral Health Team.
The Care Coordination program consists of an intensive care coordination team for youth, a separate intensive care coordination team for adults, a wrap-around team, the CHOICE program and the Multnomah Intensive Treatment Team.
The Addiction and Prevention Program works with treatment providers and community agencies to help individuals and families in Multnomah County achieve and maintain recovery. This includes managing more than 112 contracts with community-based organizations from withdrawal management and outpatient services to Substance Use Disorder services and problem gambling programs.
It also includes the Promoting Access to Hope (PATH) team and Suicide Prevention team.
Mirasol also shared that the division’s Quality Management unit “preserves the clinical integrity of services that we provide” and functions “in alignment with our mission, values and vision, and commitment to quality data-driven care, as well as out of sheer necessity.”
A recent extensive internal review required by the Behavioral Health Division’s financial agreement with the Oregon Health Authority found that “we’re in compliance with all aspects of this agreement,” said Mirasol.
Aid and Assist
At the request of the Board, presenters detailed the Aid and Assist process.
Multnomah County's Aid and Assist Program, also known as the Forensic Diversion Program, is responsible for providing clients with the necessary services, skills and psychological stability to aid and assist in their legal defense, Chief Compliance Officer and Qualify Manager Jen Gulzow explained.
In September 2022, the Mosman Order, issued by Oregon Federal District Court Judge Michael Mosman, imposed limits on Oregon State Hospital (OSH) stays for patients deemed unable to aid and assist in their own defense. Under the order, patients charged with felonies are limited to a maximum of six months in the institution, while those charged with misdemeanors are limited to a maximum of 90 days. And not all crimes qualify someone to be sent to OSH for restoration; many clients are required to be restored in the community, said Gulzow.
All clients entering the Aid and Assist program receive a community consultation or evaluation to determine their suitability for community restoration and the services needed to stabilize them to aid and assist in their defense, Gulzow said.
As a result, the County has seen dramatic rises in the number of consultations to determine if an individual is appropriate for community restoration and the services they may need to aid and assist in their own defense, the number of people under community restoration, or in the process of being restored to enable assistance in their own defense — with exceptionally short deadlines for assessments and monitoring.
Consultations increased from an average of 15 per quarter to 45 per quarter, per staff member.
Those receiving community restoration almost doubled between the first and second quarter of 2023, said Gulzow. The most recent quarterly reports showed 135 consultations were completed.
But teams are finding innovative ways to meet client needs, she said. For example, staff have begun hosting a legal skills group so clients can become closer to aiding and assisting in their defense with fewer one-on-ones.
Crisis responses, behavioral health clinics and resource networks
The Multnomah County Behavioral Health Call Center functions as a 24/7 hub of access to services and support, risk and suicide assessments, recommendations, referrals and deployment of mobile crisis services. The call center fielded more than 80,000 calls last fiscal year, Mirasol said, with 81% of calls resolved over the phone.
When Cascadia Project Respond mobile crisis response was dispatched, they were able to resolve 68% of crisis situations in the field without a higher level intervention or care. Ninety percent of callers were able to access support or services after crisis calls, which preserve placements in the community.
Sustaining the necessary level of services amid workforce shortages and increasing costs is a growing challenge for behavioral health service providers, said Mirasol, “so we’re immensely grateful for the commitment of our community partners,” including Cascadia Behavioral Healthcare, which provides mobile crisis intervention, shelter behavioral health services, an urgent walk-in clinic, and, along with Catholic Community Services, mobile crisis stabilization services.
Another crisis resource is Lines for Life/988, a crisis line for people who live in Oregon and across the country. County’s Behavioral Health Call Center works closely with Lines for Life and OHA regarding statewide and national 988 lines, said Mirasol.
The call center team developed a direct transfer line to streamline mobile crisis referrals and reduce duplication of efforts. They meet regularly with Lines for Life and OHA to focus on operational sustainability and continuous improvement.
The County also relies on and connects with local Certified Community Behavioral Health Clinics (CCBHCs), federally-designated clinics that treat mental health and substance use disorders regardless of a patient's ability to pay. Cascadia Behavioral Health and LifeWorks Northwest serve as CCBHCs in Multnomah County.
“We regularly interface with them and other service providers to connect individuals and families to services,” said Mirasol. “Referrals are based on assessments and routine crisis interface meetings are held with partners.”
While the County did not receive Measure 110 funding for its work with Behavioral Health Resource Networks — a collaborative group of service providers that work to facilitate access to treatment and recovery — it has taken on a convening role, bringing partners together monthly.
The Behavioral Health Division has assisted in establishing four Behavioral Health Resource Networks in Multnomah County, including Indigeninity and No Wrong Door, as well as networks for East County and for Latino/a/x community members.
The division also designed and launched a real-time service availability tool listing same day appointments, available beds and program criteria, added Mirasol. “We’re honored to have these partners provide services in our community.”
In early 2024, a centralized regional coordinator position, based in the Miracles Club recovery organization, was funded to help enhance the work of the Behavioral Health Resource Networks.
The presentation included an update on the Comprehensive Local Plan the Health Department is required to submit to the state.
“Oregon counties have been required to submit a comprehensive plan which provides a blueprint for behavioral health services responsive to the community,” she said.
Multnomah County’s role is to build an effective system of care and collaboration with our system partners including mental health, addiction, prevention, early intervention and treatment across the life continuum.
Changes in the system of care invariably impact the continuums, said Mirasol.
“We’re eager to not only sustain the incredible behavioral health work that happens every day in Multnomah County, but to contribute to improvements in how we approach the need in response to noticeable shifts in how mental health and substance use disorder needs are presenting themselves in the communities that we serve,” she said.
“It’s a meaningful time to be in behavioral health because the response to the need has grown exponentially since the pandemic; there’s growing attention for the support and services we provide.”
Commissioner questions and comments
Commissioner Sharon Meieran asked presenters to describe the roles of and the distinction between the Local Mental Health Authority and Community Mental Health Program.
The Board of County Commissioners serve as the Local Mental Health Authority, said Mirasol, which entails ensuring that needs are effectively met in Multnomah County. The Board also ensures that there is proper subject matter expertise to guide the work, she added.
The Behavioral Health Division presents the needs, solutions and services that address the needs of our community, “and you support us with the process of working together and approve what’s needed,” said Mirasol.
The division also has the responsibility set out in the County Financial Assistance Agreement, a commitment between OHA and Oregon counties, to provide behavioral health services.
Commissioner Julia Brim-Edwards asked about the existence of a Comprehensive Local Plan.
"The last time it was formally required by the Oregon Health Authority was in 2015, so we have one on file,” Marisol said. “It's a biennial plan, typically due every two years."
However, Marisol explained, the Oregon Health Authority requirements have fluctuated, and only recently did OHA reconnect with counties to resume having a plan in place. Multnomah County will be the first to submit an interim plan, at least, in response to a recent request.
"It's definitely appropriate for us to engage in submitting an updated plan."
"I'm going to want to hear what you think it will take, financially, in terms of staffing, and what you need from the County Commissioners, for you to do that work because we have a significant gap," Brim-Edwards said. "I look forward to our conversation about the budget and how we're going to accomplish this work."
Commissioner Lori Stegmann asked about crisis lines. “It's confusing to me because you have 988/Lines for Life, 911/the Bureau of Emergency Communication, and the Behavioral Health Call Center. Can you explain how they work together?”
“They are all separate lines, but we all coordinate and work together closely,” said Behavioral Health Manager Barbara Snow.
For example, the Behavioral Health Call Center has a direct connection with 911/BOEC and 988/Lines for Life. Both have direct backlines to the Call Center, so the County is notified when a call is transferred from 911. This is an excellent deflection point, Snow said, because we can provide behavioral health phone support and determine if we can send out a mobile crisis team instead of law enforcement.
Similarly, if 988 has done a full assessment and determined that a mobile crisis resource is necessary, they can call the County Call Center directly, which will make the dispatch call. The individual doesn’t have to go through another assessment.
Chair Jessica Vega Pederson inquired further about the requirements for submitting a Comprehensive Local Plan to the state, specifically asking whether Multnomah County differs from other counties in not having submitted a comprehensive plan to the state since 2015.
Only two counties have submitted Comprehensive Local Plans since 2015, and one of those was part of a corrective action plan, said Mirasol. She noted that most counties have plans on file from 2015.
Vega Pederson highlighted a disconnect between the role of the Board as the Local Mental Health Authority and plans submitted by coordinated care organizations and other partners to the state.
“That work, those plans happening outside Multnomah County, have never come to this board for conversation, have never come to this board for review, have never come to this board for approval,” Vega Pederson said.
“My suggestion is that this board receive the latest plan submitted there and to build on that. We need to be leading that work.”
Watch the full briefing here.